

We’re Losing Ground: Why Southeast Asia's Maternal and Newborn Health (MNH) Crisis Demands Urgent Action
Thought Piece | Singapore, 27 February 2026
In its 2025 Goalkeepers Report1, the Gates Foundation issued a stark warning: for the first time in decades, global progress on maternal mortality has stalled, at approximately 188 deaths per 100,000 live births, far above the 2030 Sustainable Development Goal (SDG) target of 70. Even more troubling, child mortality is projected to rise this year, marking the first increase this century.
This setback stems from multiple factors, with gaps in maternal and newborn care remaining the most critical. Nearly half of all under-five deaths occur in the neonatal or newborn period - the first 28 days of a life, when survival is closely linked to the health of the mother.
While global in scope, this warning is especially urgent for Southeast Asia (SEA).
Over the past three decades, the region has seen substantial reductions in its maternal mortality ratio by 59%, driven by continued government initiatives and significant funding support from global donors. Yet progress has been uneven and increasingly fragile. In certain geographies, mortality rates have stalled and are at risk of reversing, such as in Timor-Leste and Myanmar, where preventable maternal and newborn deaths remain high due to gaps in primary health care access, skilled medical staff, and postnatal support.
At a time when global health funding is declining, these already strained systems are under mounting pressure, where preventable deaths are rising not for lack of solutions, but for lack of sustained investment and coordination among funders and stakeholders.
Figure 1 - Several ASEAN countries remain off track to meet SDG 3 targets:
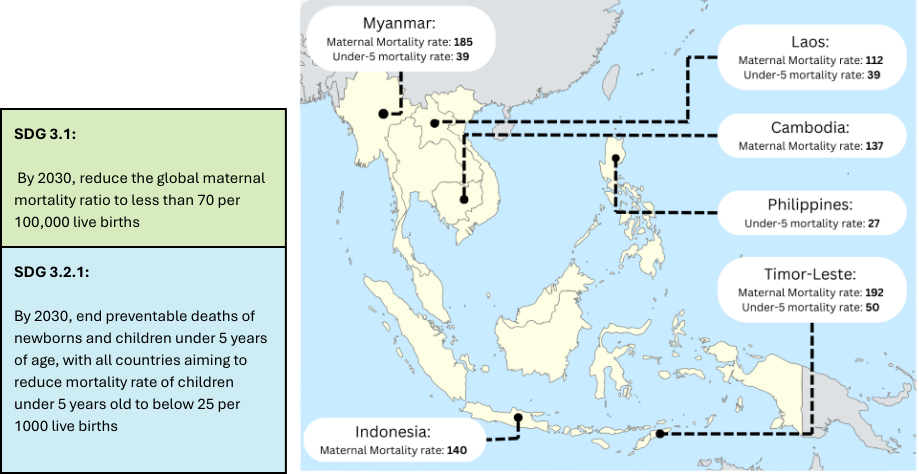
Source: WHO Global Health Observatory. Last accessed 24th February 2026; World Bank databank. Last Accessed 24th February 2026
Roots of Inequity in Maternal and Newborn Health
Despite progress in Southeast Asia, maternal and newborn health outcomes remain deeply unequal, shaped by geographic, socioeconomic, and systemic factors.
These disparities stem not only from where families live or income but from systemic weaknesses such fragile health systems and a heavy reliance on external funding.
Structural Barriers to Care
Access to maternal and newborn care varies widely across the region and even within a country. Rural and remote populations face multiple barriers including long travel distances, poor transport infrastructure, and limited availability of skilled health workers.
In Indonesia, over 70% of expectant mothers in more affluent and connected cities in Java have at least four of the six recommended antenatal care (ANC) visits during their pregnancy, compared to only 38% of mothers in its less developed regions in Papua2.
These disparities within and across countries, have direct consequences. Expectant mothers who lack access are less likely to receive preventive care, including early detection of complications, nutritional guidance, or risk screening. Newborns in these areas also face higher rates of preventable conditions such as birth asphyxia, infections, or low birth weight, contributing to ongoing neonatal mortality.
Socioeconomic Inequities
Lower information access and socioeconomic disadvantage compound geographical barriers. Women facing financial limitations have reduced access to diverse, nutrient-rich foods, supplements, and quality health information.
Ensuring sufficient nutrition for both mothers and newborns determine the trajectory of their health in the earliest stages of development. Anaemia, largely driven by nutritional deficiencies, remains a major cause of indirect maternal mortality and newborn health by elevating risks of postpartum haemorrhage, infections, and premature birth.
To counter this, the Ministry of Health in Cambodia has made iron–folic acid (IFA) supplements routinely available through antenatal care. Yet pregnant women from lower socioeconomic groups face 2.8 times higher odds of anaemia compared with those from higher-income groups3. Adherence remains particularly low among these groups, even with affordability of supplements addressed, due to fewer ANC visits and limited awareness of IFA benefits, perpetuating disparities in maternal and newborn health.
Dependence on external funding and fragile health systems
A substantial portion of MNH services in the region has historically relied on international donor support to maintain essential programmes, train health workers, and supply critical interventions.
Bilateral aid to Southeast Asia is projected to reduce up to 20% this year4, driven in part by the restructuring of major donors such as USAID and shifts in global funding priorities.
These reductions are already disrupting MNH services in the region. In the Philippines and Indonesia, multiple leading NGOs working on improving reproductive health and supporting affordable maternal health services, have had to scale back operating clinics and community outreach5. When funding contracts, services do not reduce evenly. It is rural clinics, community outreach, and lower-income families who lose access first.
Funding fragility does not merely threaten programs, it perpetuates inequities, determining which mothers and newborns have access to life-saving care. Research on health financing in Southeast Asian countries highlights that low government health spending and weak health financing arrangements impede progress toward universal health coverage, leaving underserved populations disproportionately affected by gaps in services and financial protection6.
What's Needed: Centering Communities, Scaling What Works, and Leveraging Technology
Southeast Asia’s maternal and newborn health (MNH) crisis demands urgent action, especially as international funding shrinks.
To protect lives and strengthen systems, regional philanthropic actors must invest in interventions that embrace three interconnected principles: centring communities, scaling proven solutions, and leveraging technology.
For MNH strategies to be lasting and resilient, they must put local communities at the heart of design and delivery. Local ownership and capacity development are critical, not just to expand coverage, but to ensure services are trusted, culturally responsive, and sustained beyond funding cycles. Strengthening community midwives, investing in primary health care, and building referral networks can prevent complications before they escalate. When communities are partners rather than recipients, MNH gains are embedded locally and capable of withstanding funding or other external shifts.
Southeast Asia has a strong track record of evidence-based, small-scale MNH interventions, from community-based midwifery programs to locally adapted nutrition and ANC initiatives. Yet many of these pilots remain fragmented, underfunded, or disconnected from national systems7.
Scaling what works requires bridging these gaps by integrating proven programs into government healthcare systems, securing sustainable financing, and enabling knowledge sharing on best practices that can be localised for adoption in the region.
When effectively scaled, interventions that have already shown success in pilot settings, such as community midwife networks in rural Indonesia or nutrition counselling programs in Cambodia, can achieve near-universal coverage, helping to reducing maternal mortality to levels aligned with SDG 3.1.
Thoughtfully integrated into primary health systems, technology can also strengthen community-based care, extend reach to underserved populations, and help scale proven solutions effectively.
Digital tools support frontline workers with real-time decision-making, track high-risk pregnancies, and enable mothers with health information. In Vietnam, SMS push notifications remind expectant mothers of ANC visits, nutrition, danger signs, and postnatal care, improving awareness and uptake, especially in remote communities8.
Beyond communication, digital innovations address screening and accessibility challenges. Portable ultrasound devices, point-of-care diagnostics, AI-supported risk assessments, and telehealth platforms enable early detection of complications and timely specialist consultations.
The Way Forward
Southeast Asia is not losing ground in MNH for lack of solutions, but for lack of sustained commitment to deepen and scale interventions.
Maternal mortality has plateaued in several countries, neonatal deaths remain stubbornly high in underserved communities, and workforce shortages are widening gaps between urban and rural care. As global financing contracts, the risk of steady backsliding increases.
Asian philanthropy, with its growing capital and influence, is uniquely positioned to reduce dependence on volatile external funding and shape a more self-reliant future. By aligning capital with evidence and strengthening locally led systems, regional funders can move beyond short-term preservation, toward long-term resilience and equity.
Asia Community Foundation’s Maternal and Newborn Health (MNH) Fund brings together regional philanthropists to co-invest in community-based care, scalable system strengthening, and locally led innovation across Southeast Asia.
We invite funders to join us in building resilient, regionally anchored solutions that protect mothers and newborns, regardless of shifting global aid cycles.
For more information, please reach out to Saleha Ali, saleha.ali@asiacf.org
- Gates Foundation (2025) 2025 Goalkeepers Report: We Can't Stop at Almost. Bill & Melinda Gates Foundation. Available at: https://www.gatesfoundation.org/goalkeepers/report/2025-report/ (Accessed: 26 February 2026).
- Health Development Policy Agency (Badan Kebijakan Pembangunan Kesehatan/BKPK), Ministry of Health of the Republic of Indonesia (2024) SKI Thematic Report: Indonesian Health Survey (SKI) 2023. Jakarta: Ministry of Health of the Republic of Indonesia. Available at: https://www.badankebijakan.kemkes.go.id/en/laporan-tematik-ski/ (Accessed: 26 February 2026).
- Buanasita, A., Sumarmi, S., Mahmudiono, T., Melaniani, S., Salim, L.A., Sokvy, M. and Sari, N.M. (2025) 'Adherence to iron supplementation and associated factors among pregnant women in Cambodia: insights from the 2021–2022 Demographic and Health Survey', Narra J, 5(2), e1659. https://doi.org/10.52225/narra.v5i2.1659
- Dayant, A., Stanhope, G., Rajah, R., and Buckley, H. (2025) Southeast Asia Aid Map: 2025 Key Findings. Sydney: Lowy Institute. Available at: https://seamap.lowyinstitute.org/analysis/2025/key-findings/ (Accessed: 26 February 2026).
- Centre for Asian Philanthropy and Society (2025) Maternal and Child Health in Asia: How Asian Philanthropy Can Meet the Moment. Hong Kong: Centre for Asian Philanthropy and Society. Available at: https://caps.org/research/maternal-and-child-health-in-asia-how-asian-philanthropy-can-meet-the-moment/ (Accessed: 26 February 2026).
- World Health Organization (2024) Strategic Framework for Improving Newborn and Child Health in the South-East Asia Region (2024–2030). New Delhi: WHO Regional Office for South-East Asia.
- Dao, B.T.T., Trinh, H.T., Lai, P.H., Elsner, T., Kane, S., and Nguyen, L. (2023) 'A cluster randomised control trial of an SMS-based intervention to promote antenatal health amongst pregnant women in a remote, highland region of Vietnam', Healthcare, 11(17), 2407. https://doi.org/10.3390/healthcare11172407